Note: Your progress in watching these videos WILL NOT be tracked. These training videos are the same videos you will experience when you take the full ProACLS program. You may begin the training for free at any time to start officially tracking your progress toward your certificate of completion.
The term asystole simply refers to an absence of ventricular activity, which means the patient will exhibit no discernible electrical activity on an ECG readout. In most cases, asystole is a lethal arrhythmia and survival is extremely rare.
In this lesson, we'll look at an ECG readout for a patient in asystole, tackle those H's and T's and provide some corresponding information about their diagnostic use, and at the end of the lesson, provide some information on asystole and technical problems.
Asystole is a cardiac standstill where there is no discernable electrical activity. It Is represented by a straight flat, or almost flat, line on an ECG.
Warning: However, do not rely on an ECG alone for your diagnosis of a patient in cardiac arrest. It's a good idea to always confirm it clinically, because what appears to be a flat line on the ECG can also be caused by a loose ECG lead.
Now let's take a look at an ECG for a patient in asystole.
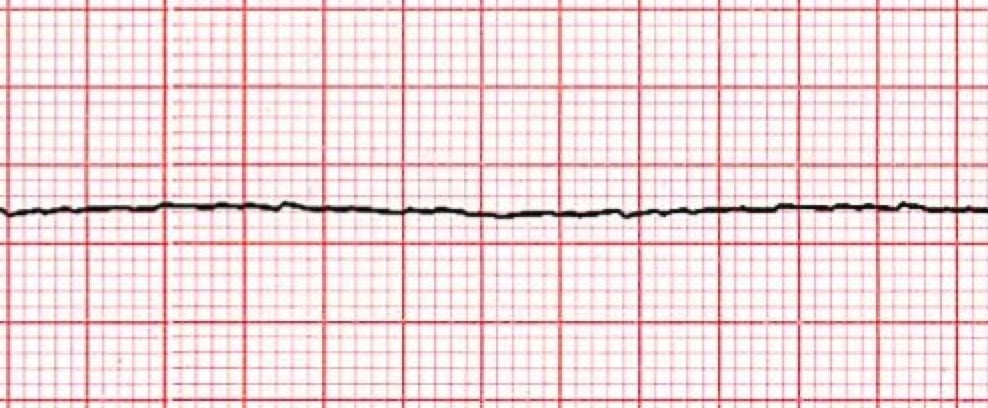
*Asystole ECG for Adult Patient
1. The Heart Rhythm
The first thing you'll want to look at is the heart rhythm. Does the heart rhythm look regular? Or does it look irregular? In the ECG above, there is no heart rhythm.
2. The Heart Rate
Next, you'll want to look at the heart rate of the patient. What is the patient's heart rate? Is it normal? Or is it too slow or too fast? In this case, there is no rate and no pulse.
3. P-Wave
After looking at the heart rate, check to see if the patient's P-waves look normal by asking yourself the following few questions.
- Are the patient's P-waves present? No, making any other questions about QRS non-applicable. However, in some cases, a small P-wave can be seen but it isn't followed by any other waveforms.
Pro Tip #1: If you notice these small P-waves on the ECG that aren't followed by any other waveforms, this can mean that, in rare cases, the atrial pacemaker may be trying to send an impulse but has no ventricular reaction.
4. PR Interval
Next, look at the PR interval on the patient's ECG readout and ask yourself the following questions:
- Is the PR interval normal, meaning between .12 and .20 seconds or is it contained within one large square on the readout? The answer is no, because there isn't a PR interval.
- Is the PR interval constant? Again, this in non-applicable since there isn't a P-wave.
5. QRS Complex
The last thing you should look at to determine if the sinus rhythm is normal or not is the QRS complex and ask yourself these questions while you do:
- Is the QRS interval less than .12 seconds? No. In fact, there is no evidence of a QRS complex, making any other questions about QRS non-applicable.
So, what is your cardiac interpretation? Based on these questions and on the findings from the ECG readout above, it would appear that this patient is in asystole. Because there is no myocardial, electrical, or mechanical activity, there is no pulse and no circulation of blood and oxygen.
Pro Tip #2: Asystole is most commonly seen following a period of unconverted ventricular fibrillations or ventricular tachycardia. And while asystole is most commonly seen after extended, untreated, and sudden cardiac arrest, it can also be caused by reversible conditions outlined below.
The most common reversible causes of asystole can best be remembered by keeping in mind the H's and T's.
H's and T's
The following H's and T's are designed to help you identify (and easily remember) potentially reversible causes of cardiac arrest or factors that may be complicating your resuscitative efforts.
The H's |
The T's |
| Hypothermia | Toxins |
| Hyper or hypodalemia | Tamponade |
| Hypoxia | Tension pneumothorax |
| Hydrogen ion (acidosis) | Thrombosis (pulmonary) |
| Hypovolemia | Thrombosis (coronary) |
A Word About Asystole and Technical Problems
Asystole is a specific diagnosis. However, a flat line is not. The term flat line is nonspecific and can be the result of several possible conditions, including the absence of cardiac electrical activity, lead or other equipment failure, and/or operator error.
Some defibrillators and monitors will signal the operator when a lead or other equipment failure occurs. However, some of these problems do not apply to all defibrillators.
For a patient with cardiac arrest and asystole, you should quickly rule out any other causes of an isoelectric ECG, such as:
- Loose leads or those that are not connected to the patient or defibrillator/monitor
- No power source to the defibrillator/monitor
- Signal gain (amplitude/signal strength) that is too low















